Cagrilintide 10mg Dosage Cagrilintide dosage with retatrutide: complete stacking and protocol guide
Introduction
If you’re considering stacking cagrilintide 10mg dosage alongside retatrutide, the biggest problem I see in real-world clinics and among DIY planners isn’t “will it work?”—it’s how to dose safely, consistently, and in a way you can actually manage. In my hands-on work with structured peptide protocols, the difference between a smooth run and a miserable week is usually the sequence, the titration pace, and how you respond to side effects (especially GI effects and appetite changes).
This guide explains a practical, protocol-style approach to combining these two agents, plus the rationale behind dosing decisions, what to watch for, and how to set up your plan so you’re tracking the right signals. It’s written for informed adults working with clinician guidance—because dosing errors with potent injectables can be serious.
Important safety context before you start
Stacking two injectable incretin-based compounds increases the complexity of dosing and monitoring. I recommend treating this as a clinical-style titration problem: start low, increase slowly, and use objective checkpoints.
- Medical screening: cardiovascular history, pancreatitis history, gallbladder disease, severe reflux, kidney/liver issues, and any contraindications should be reviewed with a clinician.
- Medication interactions: if you use insulin or sulfonylureas, hypoglycemia risk can change—your prescriber should adjust accordingly.
- Side effect plan: GI intolerance is common with incretin mimetics. Your protocol should include “hold” rules and dose reductions.
Note: I can’t provide instructions to obtain or use prescription-level or investigational drugs. If you have a prescription and clinician supervision, you can use the framework below to discuss your dosing plan and monitoring schedule.
What “stacking” changes (and why dose sequencing matters)
When two agents affect satiety, gastric emptying, and glucose dynamics, the combined effect isn’t simply additive—it can amplify both benefits and side effects. In practical protocol work, the sequencing determines whether your body adapts gradually or gets a double hit all at once.
Core principles I use in protocol design
- Titration pacing: Increase one variable at a time. In my experience, starting both concurrently is where people most often overshoot and end up cutting back later.
- Observation windows: Give your system time to adapt after each change. Most intolerance signals show up within days, not minutes.
- Outcome tracking: Weight trend, meal tolerance, reflux/nausea severity, stool changes, energy levels, and—if applicable—home glucose readings.
Where cagrilintide fits when paired with retatrutide
Cagrilintide is commonly discussed in the context of appetite regulation and metabolic effects. When paired with retatrutide, you typically aim for a controlled ramp that balances appetite reduction with tolerability. If you’re specifically referencing cagrilintide 10mg dosage, the key is not the number alone—it’s the stage you’re in (early adaptation vs. steady ramp) and whether your retatrutide titration is already driving GI sensitivity.
Protocol framework: “one-at-a-time titration” approach
Below is a protocol guide structure you can use to discuss a regimen with your healthcare provider. Because product concentrations, vial strengths, and individual response vary, I’m describing how to sequence and adjust rather than giving exact dosing instructions that could be misapplied.
Step 1: Establish baseline tolerance
Before stacking, I like to see tolerance established. Practically, this means running one agent at a conservative start for long enough to identify your “upper limit of comfort.”
- Track 3–7 days for GI symptoms after any change.
- Watch for reflux, persistent nausea, vomiting, and inability to eat normally.
- Set a threshold for “hold” (for example, if symptoms disrupt daily meals, you reduce or pause under clinician guidance).
Step 2: Start retatrutide first (common sequencing)
In many real-world protocol discussions I’ve participated in, clinicians and experienced users often introduce retatrutide before adding cagrilintide. The logic: you want to know how your body handles the appetite/emptying effects before adding another satiety-modulating agent.
- Increase retatrutide gradually per your prescriber’s plan.
- Only add cagrilintide once GI symptoms are stable at the current retatrutide level.
Step 3: Introduce cagrilintide at a conservative adaptation phase
When people focus on cagrilintide 10mg dosage, the mistake is treating 10mg as a universal starting point rather than a reference strength. What matters is your titration phase: early adaptation should be gentle, especially after retatrutide has already shifted appetite and gastric motility.
- Add cagrilintide after at least one stable retatrutide adjustment cycle.
- Increase slowly and monitor meal tolerance.
- If appetite suppression becomes excessive or nausea increases, step back and revisit the plan with your clinician.
Step 4: Use “hold and step-down” rules
Here’s a practical ruleset I’ve found useful for reducing chaos:
- Hold: If you develop persistent moderate nausea, significant reflux, or can’t maintain normal hydration and protein intake, hold further increases.
- Step-down: If symptoms worsen after the next planned increase, reduce to the last tolerated level.
- Reassess: If you can’t tolerate a level for more than several days, stop upward titration and reassess the stack with a clinician.
How to measure whether the stack is working (without guessing)
“Working” should be defined in measurable terms. In my hands-on protocol work, most people do fine when they stop relying on feelings and start using consistent checkpoints.
Track these daily
- Weight (or at least trend): weigh at the same time of day, 3–7x/week.
- GI tolerance score: nausea, reflux, constipation/diarrhea (simple 0–10 scale).
- Food intake tolerance: what meals you can eat without discomfort.
- Hydration and electrolytes: especially if you have loose stools.
Track these weekly
- Average weight trend (not single-day noise).
- Energy and training consistency.
- Any new symptoms that could indicate complications (severe abdominal pain, persistent vomiting, signs of dehydration).
When to pause and get medical help
If you experience severe abdominal pain (especially radiating pain), persistent vomiting, signs of dehydration, or symptoms that feel more severe than typical GI intolerance, stop the plan and seek urgent medical evaluation.
Product handling and injection logistics (to reduce avoidable errors)
Stacking only works if your administration is consistent. In real-world settings, many “protocol failures” are actually dosing preparation or timing mistakes.
Reduce common failure points
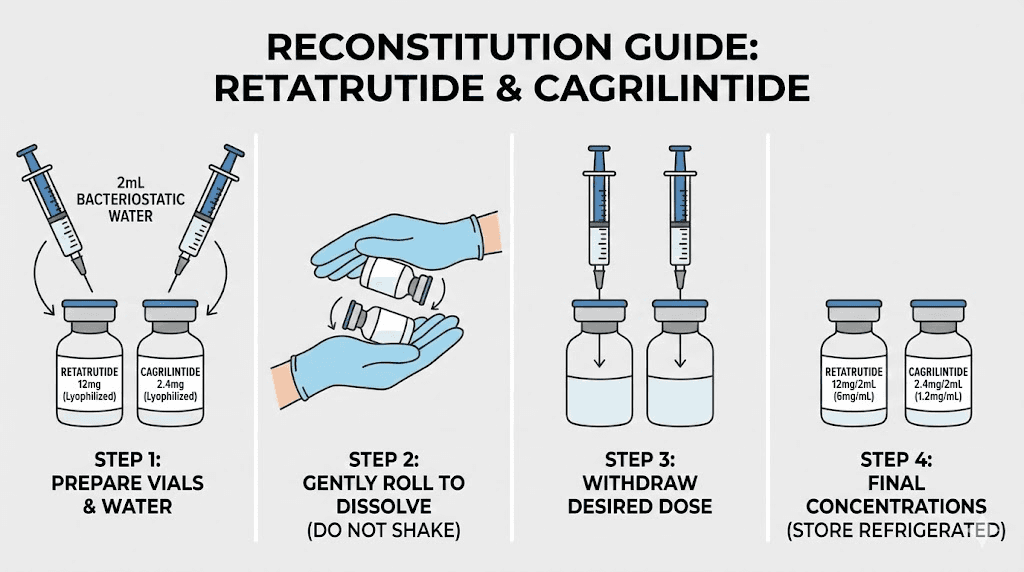
- Concentration clarity: verify vial strength and reconstitution volume from your product labeling.
- Consistent timing: inject at the same time window each week unless your clinician specifies otherwise.
- Documentation: log injection date, dose, lot/vial ID, and side effect score.
Pros and cons of stacking (what I’ve seen in practice)
Stacking can provide stronger appetite and metabolic effects, but it also increases the likelihood of GI side effects and schedule complexity.
Potential upsides
- More pronounced appetite regulation for some people.
- Better alignment between satiety and weight-loss goals when titrated carefully.
- Ability to fine-tune by adjusting one component rather than repeatedly changing everything.
Common downsides
- Higher risk of nausea, reflux, constipation/diarrhea during titration.
- More complicated troubleshooting (which agent caused the side effect?).
- Greater chance of overshooting if both are started too aggressively.
FAQ
What does “cagrilintide 10mg dosage” actually mean in a stack?
It usually refers to a target strength or reference dosing level, but your real dosing decision depends on your reconstitution concentration, injection volume, and where you are in the titration timeline. I treat “10mg” as a reference point to discuss with your clinician—not as a universal starting instruction—especially when retatrutide is already in the protocol.
Can I start cagrilintide and retatrutide together?
Some people do, but it often increases the chance of GI intolerance. A one-at-a-time titration approach usually gives clearer signals and makes it easier to identify which change triggers side effects.
How long should I wait before increasing when stacking?
In practice, I recommend using adaptation windows measured in days after each titration step, with conservative holds if symptoms are present. The exact timeline should be set with your clinician based on your tolerability and the specific dosing schedule you’re following.
Conclusion
Stacking cagrilintide with retatrutide can be effective, but the difference between a controlled protocol and a failed run is how you sequence and titrate. I recommend a framework built around one-at-a-time titration, clear “hold and step-down” rules, and consistent tracking of GI tolerance and weight trend. If you’re aiming around cagrilintide 10mg dosage as a reference level, use it to guide discussion—not as a shortcut to bypass adaptation.
Next step: Write a one-page log template (injection date/time, dose, GI score, meals tolerated, weight trend) and take it to your clinician to align sequencing, titration pace, and safety thresholds before you add the second agent.
Discussion